In recent years, hospitals have become increasingly engaged in mergers, affiliations, downsizings, and creation of health care networks. This has led to an approximate 25%reduction in the number of hospital beds with an increasing proportion of their inpatient coming from the unpredictable fluctuating demands of emergency admissions rather than planned elective patients during the last 20 years. Finding a suitable bed would, thus, become a scarce commodity in the Indian context considering their average bed population ratio of 6.8:10000. Moreover, the cost of making a new bed available varies between Rs. 50,000 to Rs. 100,000 along with the additional costs of their maintenance.
Lack of beds in such a scenario would result in a longer boarding time (48.7 minutes) for the hospitals with more than 50,000 or more annual visits in comparison to the ones with less than 20,000 annual visits (24.1 minutes) as per the National Health Survey, 2018. Due to this, hospital managers have been under constant pressure of reducing the bed capacity to increase their occupancy rates in the name of operational efficiency. This would require our health systems to add capacity without construction in order to get ahead of demand while maintaining or improving patient outcomes and satisfaction with the following action points.
Using data analytics for a better bed allocation:
Bed occupancy as a measure has shown a recent increase where hospitals with average bed occupancy levels above 85% can expect to have regular bed shortages, periodic bed crises, and increased numbers of acquired health care infections.
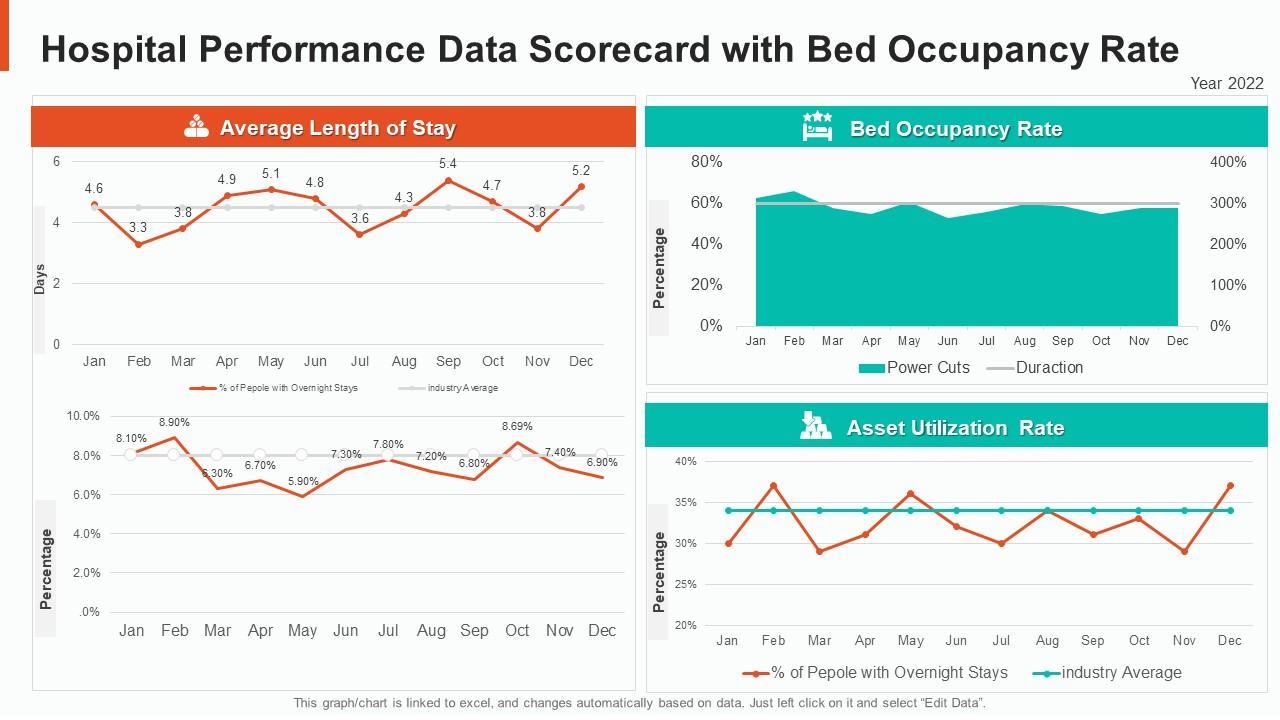
An average length of hospital stay (ALOS) is defined by the inpatient stay requiring continuous and active medical, nursing, or paramedical treatment which couldn’t be provided through external care, day care, or outpatient care.
ALOS = No. of inpatient days
Number of discharges and deaths in that month
Bed occupancy ratio (BOR) is the average daily number of persons hospitalized per
thousands of populations. It reflects efficiency in the use of hospital beds where a hospital is
considered to be operating efficiently at BOR of 80–90%
BOR = No. of inpatient days × 100%
No. of days in a given month
A large number of bed for an economically developed country would imply a larger volume of hospital utilization though it is unlikely that these two trends might correlate. With the help of such indices, the hospitals would be able to identify key process and outcome metrics for addressing the dearth of beds across departments. This can help increase transparency and measure impact by taking advantage of the following predictive capabilities:
- A 24 – hour discharge dashboard to show the patient discharge plan throughout the hospital. Such data would help the team identify patients which are most likely to be discharged in order to ensure that they aren’t taking up beds.
- An annual capacity management assessment to help healthcare facilities differentiate a year-long capacity problem from seasonal spikes.
Improving the efficiency of bed allocation with staffing patterns:
The scrutiny of internal healthcare systems along with their organizational factors has been attributable to the significant portion of delayed discharges. This includes patients waiting for results of investigations, consultant’s input, assessment from specialist health care providers, transport, and pharmacy services as typical inefficiency or provision failures. Directing inpatient flow is knowing where and when bed staff needs to be deployed in the hospital’s support services. This would require assigning and equipping the staff efficiently for better patient care with a reduced average length of stay. Facilitating earlier discharge in this way would eventually increase the bed capacity of a hospital which may, otherwise, severely affect the admissions and discharge procedure.
Process improvement:
Most of the hospital beds remain occupied from the high volume of patients stay which subsequently increases the length of time required to manage patients’ complaints. The type, extent, and quality of health care service in such a case would affect bed utilization in a number of ways. The resulting inefficiency gaps in the demand-capacity ratio of available beds and unnecessary delays in bed turnaround processes would, therefore, need to be addressed with the following action points:
- Tracking the bed turnaround time – i.e. elapsed length of time between patient 1 leaving and patient 2 arriving.
- Improving communication between the services team who cleans the beds and the allocated nurse assigning new patients in those beds
- Timely recognition and response to the bed status signal for maintaining an uninterrupted process flow.
- Creating a ‘Transitional Care Area’ to transfer the stable patients from their monitored bed and, thereby, increasing their capacity for new patients.
Flexibility in bed usage is considered to be a key concept for the efficient management of hospital beds. Eliminating such long hospital stays would subsequently decrease the hospital costs and the risks of no socomial infection, and spare available bed resources for patient reporting.
Managing patient flow to free up bed capacity:
The level of risk to both patients and hospital is a function of the rate at which new emergency patients arrive at the hospital, the rate at which emergency patients are subsequently discharged, and the daily available bed capacity. This require the standardization of decision process for the patient placement, bed utilization, and appropriate allocation of resources which would lead to higher bed occupancy through the following points:
- An evidence based triage assessment such as the Emergency Severity Index (ESI) or a triage acuity scale would help determine the patient acuity and priority of care at triage. Following this, the patients can either be moved to an ED room or may have to wait for care, if not critically ill.
- Developing an Early Team Evaluation (ETE) protocol to determine which patients may be treated and wait safely in a chair rather than a hospital bed.
By using this preventive strategy, hospitals would be able to reduce patient’s length of stay and their high bed occupancy rate. This would eventually help in the business excellence for healthcare professionals as a management tool for improving the operational efficiency of healthcare services and their use of existing facilities without compromising on the quality of care.
Enrol with Certification in Business Excellence for Healthcare professionals for further information
Use Coupon code: ASTRONEC20 to get exciting offers!
References:
file:///D:/content%20astron/bed%20occupancy/Monitoring%20Hospital%20_%20Bed%20Oc
cupancy%20Rate%20_%20Hospital%20Occupancy%20Rate.html
https://www.cdc.gov/nchs/data/factsheets/factsheet_nhcs.htm
Majeed, M.U., Williams, D.T., Pollock, R., Amir, F., Liam, M., Foong, K.S. and Whitaker, C.J., 2012. Delay in discharge and its impact on unnecessary hospital bed occupancy. BMC health services research, 12(1), pp.1-6.
National Accreditation Board for Hospitals (NABH) standards, 5 th edition, 2020 Qureshi, W. and Hassan, G., 2014. A five year retrospective study of bed utilization trends in a tertiary care teaching institution. JK Science, 16(3), p.119.


No comments:
Post a Comment